










fizkes/Shutterstock
The term “long COVID” is used to describe symptoms or illness that continue for more than four weeks after a positive COVID test or the original onset of symptoms. Some examples include an ongoing loss of taste or smell, debilitating fatigue, and even sustained damage to the heart or brain.
Long COVID can seriously affect people’s quality of life and ability to work. And there are no proven treatments, meaning that we may be facing a wave of disabilities with little we can do to help.
But in a new paper, my colleagues and I report that referrals for more severe cases of long COVID have dropped over the past year, despite large waves of delta and omicron infections.
In this research, we looked at referrals to the long COVID clinic at the Cambridge University Teaching Hospital between August 2020 and June 2022. These patients are on the more severe end of the long COVID symptom spectrum, having been referred following assessment by a team of specialists after at least five months of symptoms.
We found a 79% drop in the number of patients being referred to the clinic from August 2021 to June 2022, compared with August 2020 to July 2021.
Our study is naturally limited by its small size. It includes data from only 145 patients, and these people are local to the area around Cambridge. I’m looking forward to seeing whether other research groups from clinics around the world are seeing similar trends.
Vaccination and long COVID
There could be other reasons for the positive trend that we’ve witnessed, but the timing suggests that vaccination is the most likely explanation. The decrease in referrals begins in August 2021, around five months after the British population started receiving second doses of COVID-19 vaccines.
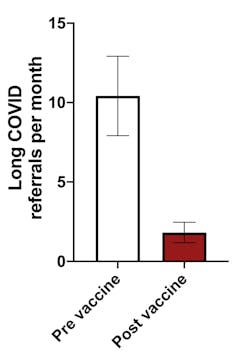
Based on data from Krishna et al., 2022, Author provided
This graph, showing the average number of long COVID referrals before and after this point, highlights a clear link between the two.
There is some evidence already to suggest that immunity gained from vaccination protects against long COVID, though the size of the effect differs between studies.
For example, one study from the US showed a 15% reduction in long COVID symptoms after vaccination, a study from the UK saw a 50% reduction, while one study from Israel found vaccination was associated with no long COVID symptoms at all.
The reason for these differences will have a lot to do with testing methods. For instance, how long after COVID-19 did the researchers survey symptoms? What symptoms constitute long COVID, and how severe do these symptoms need to be to qualify?
While it’s difficult to pin down the degree to which vaccination reduces long COVID symptoms, we believe it has played a key role in the reduction in new referrals we’ve seen in our clinic. The fact that other groups, using different measuring techniques, have also observed this association is very reassuring.
Reinfections
We’re now in a phase of the pandemic where reinfections are increasingly common and will probably soon constitute most infections.
This leads us to an important question: does reinfection carry the same risk (or even an increased risk) of long COVID, compared with previous infections? If it does, we would be in big trouble as each reinfection will lead to more and more people with long COVID, eventually overwhelming health services.
But this assumes that previous infections have no bearing on long COVID risk. In reality, we need to consider other factors.
First, there’s the possibility that some people are predisposed (and likewise, not predisposed) to long COVID. Studies have already found a range of factors that predict long COVID risk, such as previous infections with other viruses, like Epstein-Barr virus.
I haven’t yet seen a study linking long COVID to genetics, but I would be surprised if there are no genetic factors that predispose a person to long COVID.
If some people are indeed predisposed to long COVID, then these people will be more likely to develop long COVID from a first infection, while others will never get long COVID, even after repeated infections. Multiple COVID infections may therefore not be that risky.

Prostock-studio/Shutterstock
Another possibility is that immunity to SARS-CoV-2 (the virus that causes COVID-19) may protect against long COVID. Each subsequent infection would then have a reduced chance of causing long COVID compared with the first infection as immunity builds up.
While the trend we observed would support this (in that a much greater number of COVID cases later on would have been reinfections), it’s not yet clear if immunity from a prior infection protects against long COVID, nor whether reinfections with SARS-CoV-2 hold the same risk of long COVID as a primary infection.
Research from the US suggests that the risk of long COVID accumulates with every reinfection, so more infections mean higher risk. However, the definition of long COVID in this study is very broad, including any symptoms at six months. It’s also a preprint, meaning the results have not yet been reviewed by other scientists.
The data does suggest, however, that reinfections add less to the risk of long COVID than the initial infection. So while each reinfection is not without risk, the risk may be somewhat less compared with a first infection.
Read more:
Long COVID: vaccination could reduce symptoms, new research suggests
We’re certainly not out of the woods yet. We know that immunity to SARS-CoV-2, both from vaccination and prior infections, wanes over time. Long COVID rates may start creeping upwards as immunity across the population drops. We will need to monitor this situation carefully and continue to focus on booster vaccines.
![]()
Ben Krishna does not work for, consult, own shares in or receive funding from any company or organisation that would benefit from this article, and has disclosed no relevant affiliations beyond their academic appointment.