










Ian Davidson/Alamy
In February, Prime Minister Boris Johnson said the public would have to get used to “living with COVID”, and announced the phasing out of all COVID-related restrictions over the following months. For many people, life since then has begun to return to something resembling normal.
Of course, there are some notable differences to pre-pandemic times, with a huge increase in working from home, and worryingly, many people still suffering from long COVID. But in most respects, you could be forgiven for thinking the pandemic was over.
Yet, over the past few weeks, there have been indications that a new wave of COVID is coming. The latest data from the Office for National Statistics’ (ONS) infection survey suggests that around 1.7 million people in the UK had COVID in the week ending June 18 – an increase of over 80% in the previous three weeks. Given the infection survey data is published with a delay of at least one week, these figures almost certainly underestimate the number of cases today.
COVID cases across the UK are rising
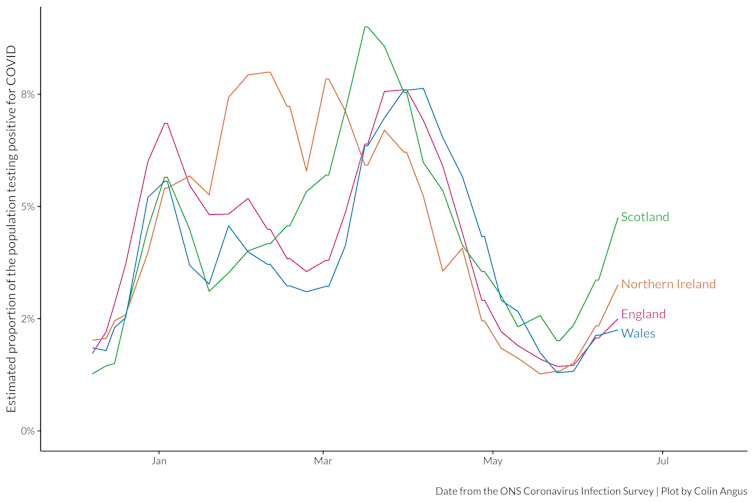
One significant change in the last few months has been the end of free mass testing, which stopped in April. While this was inevitable at some stage because of the significant costs involved, it has taken away one of the UK’s key early warning systems.
In the past, an increase in positive tests in the community has been among the first signs that a new wave was coming. Without this, we may not realise the seriousness of a new variant until it’s already well established and people start turning up in hospitals in increasing numbers.
BA.4 and BA.5
Two new omicron variants, BA.4 and BA.5, are making up most of the infections in the current wave. Both of them are more transmissible than BA.2, the previously dominant variant. The evidence is still unclear on whether these variants are more or less severe than earlier forms of omicron, but the UK Health Security Agency (UKHSA) has classified them as “variants of concern”.
The latest hospital data shows that the number of new COVID patients (a combination of new admissions and people who catch COVID in hospital) in England is rising. In the most vulnerable age groups (65 and over) these figures are at almost two-thirds of the January peak seen during the initial omicron wave.
Rate of new COVID hospital admissions in England by age
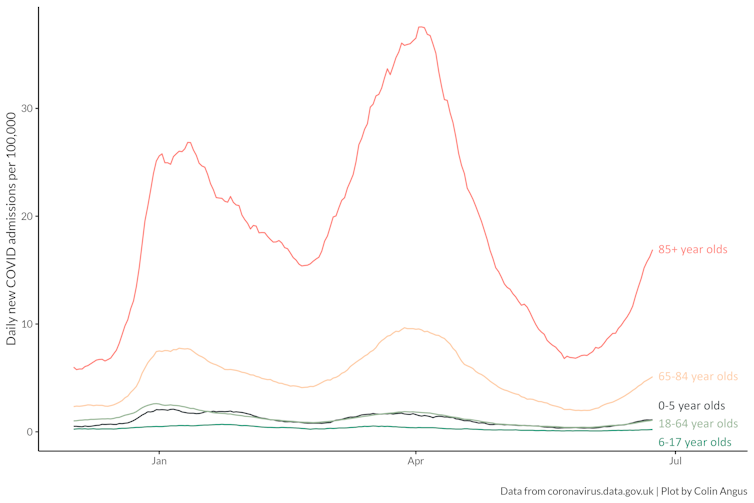
The situation is most acute in the north-west of England, where there are currently around 200 new COVID admissions every day. The north-west was also one of the worst affected parts of the country in terms of hospital admissions during the BA.1 and BA.2 waves.
The key question at this stage is how long this increase will carry on for. Without the early warning system of mass testing, it’s hard to know. Ultimately, this wave will start to subside when the growth advantage of the new variants comes up against the wall of immunity put up by vaccinations and previous infections.
Although we’ve done an excellent job of getting initial doses of COVID vaccines in arms in this country, a combination of immunity waning over time and the fact that newer variants are generally better at overcoming this immunity means that this wall is not as strong as it once was.
There are, however, a few reasons to be cautiously optimistic. South Africa, which has often been a bellwether for new variants, and where BA.4 and BA.5 were first identified, saw a much smaller wave as a result of these variants, with relatively few hospitalisations and deaths compared with previous waves. Portugal was one of the first European countries to see a BA.4/5 wave and, while it did see a significant increase in hospital admissions, case numbers now appear to have begun to fall without reaching the same severity as previous waves.
Some cause for concern
Even if the BA.4/5 wave isn’t as big as earlier waves, there are two major concerns. The first is the pressure already placed on the NHS, which has been stretched to the limit by the events of the last two years. Ambulance waiting times are at record levels, as are A&E waiting times, with over one-quarter of patients waiting more than four hours to be seen. This comes alongside a huge backlog of operations and other types of medical care that were delayed during the pandemic. Even a modest BA.4/5 wave is only going to add to these pressures.
The second issue is the growing number of people with long COVID. As many as 1.4 million people in the UK report symptoms that affect their day-to-day lives. And these figures are from May, before infections started rising again.
Read more:
Long COVID: female sex, older age and existing health problems increase risk – new research
So what can we do? If you were taking precautions earlier in the year that you’ve since dropped, it would be wise to think about picking these up again. These include things like wearing a mask in crowded places, not meeting people if you have any symptoms, and testing if possible if you’re feeling unwell or are going to spend time with someone who is vulnerable. The UKHSA also suggest meeting other people outdoors or in well-ventilated places.
To help reinforce our protection against these new (and future) variants, there might be merit to bringing the autumn booster campaign, which will offer a fourth dose to people over 65 and other more vulnerable groups, forward. It may also be worthwhile to consider offering fourth doses to younger age groups soon, and additional boosters to the most vulnerable groups.
The tide of the pandemic is going out. But as with any receding tide, there will always be the odd bigger wave that can catch you out if you’re not careful. The end of mass testing and threats to the future of the invaluable ONS COVID infection survey make it more likely that these waves will catch us unprepared. The parlous state of the NHS and the threat of long COVID mean we shouldn’t be complacent to the potential threat of this, or subsequent waves, even as the tide continues to go out.
![]()
Colin Angus does not work for, consult, own shares in or receive funding from any company or organisation that would benefit from this article, and has disclosed no relevant affiliations beyond their academic appointment.